

Background
● People who experience sexual trauma (ST), such as unwanted sexual contact, may also experience severe mental health struggles as a result1
● Dialectical Behavior Therapy (DBT) and Cognitive Behavioral Therapy (CBT) have shown efficacy in treating those who have experienced sexual trauma2, 3
● Additional research is needed on the effectiveness of these treatments in real-world settings
Research Questions & Hypotheses
RQ1: Do DBT and CBT patients who have experienced sexual trauma report improvement in symptomatology over time?
RQ2: Do DBT and CBT patients who have experienced sexual trauma report significantly slower improvement in symptomatology over time than DBT and CBT patients who have not experienced sexual trauma?
H1: DBT and CBT patients who have experienced ST will report a significant improvement in treatment outcomes over time.
H2: DBT and CBT patients who have experienced ST will report outcomes that do not significantly differ over time compared to DBT and CBT patients who have not experienced ST
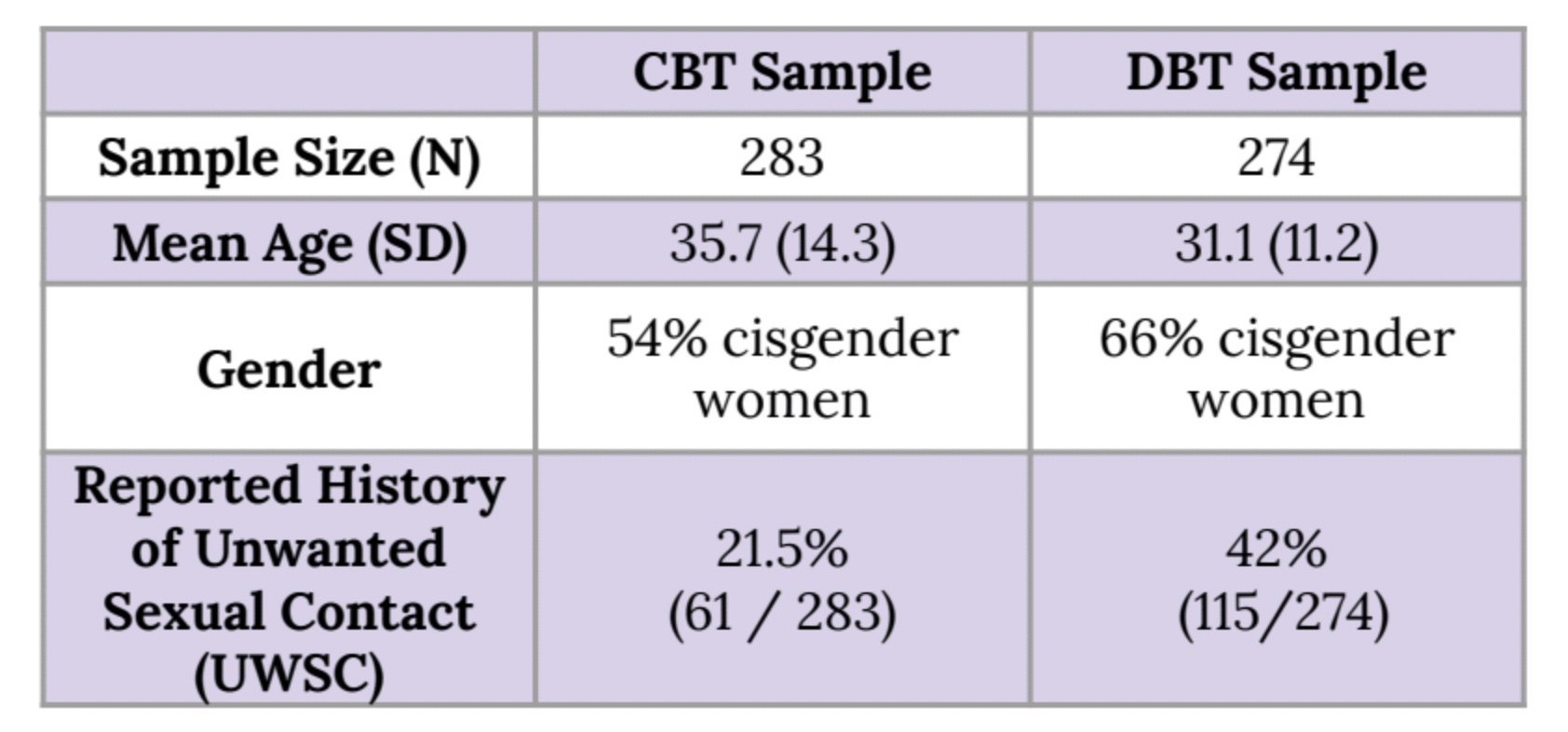
Method
Measures: PCL-5, GAD-7, PHQ-9, WSAS, MHC-SF-14;
Analysis: Multilevel Modeling
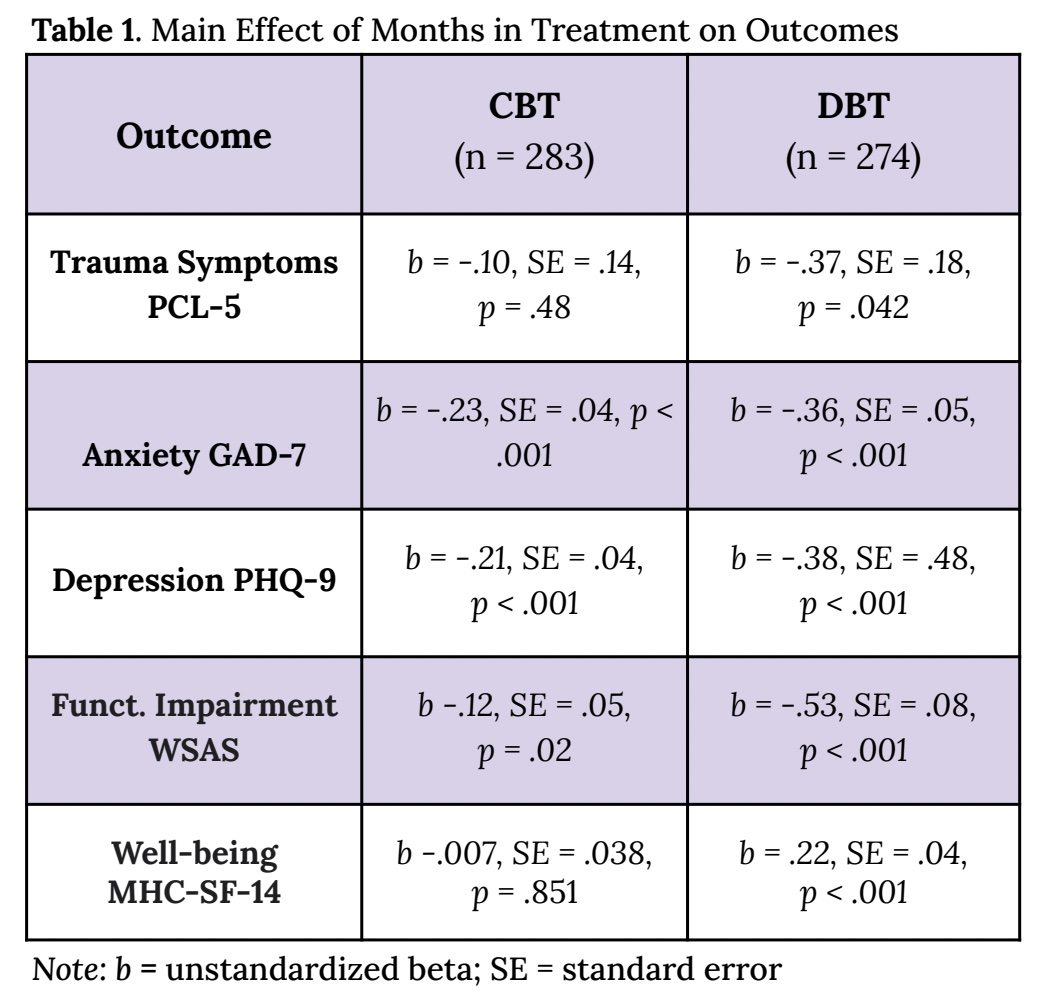
Results
H1 ~Supported: For DBT patients, improvements over time were reported across all outcomes. For CBT patients, improvements were reported for depression, anxiety, and functional impairment.
H2 Supported: Improvement in outcomes did not differ for those with a history of ST vs. those without ST for all outcomes across the DBT & CBT groups except:
– PCL-5 scores at baseline were more severe for those with ST than those without (5.4 points higher for CBT group; 17.6 points for DBT group)
– Scores improved at a faster rates for those with ST vs. those without ST (CBT: b = -.54, SE = .21, p = .013; DBT: b = -.67, SE = .27, p = .012)
Discussion
● For ST patients, both treatments showed reductions in traumatic, depressive, and anxiety symptoms as well as functional impairment
● With a few exceptions, neither therapy group’s improvement rates were significantly different for patients with or without a history of ST
● Those with ST had more acute trauma symptoms at intake, but they recovered more quickly than those without ST
● For clinicians, this provides evidence that DBT and CBT may be reliable therapy modalities for those with a history of ST
Strengths
● Real world outpatient sample
● Use of multiple scales to track symptoms over time at multiple timepoints
Limitations
● Lack of a control group
● Limited generalizability
● Categorization of sexual trauma variable
Future Research
● Use of a control group to compare the effects of the treatment model
● Investigate emotional dysregulation change over time based on the treatment model
Research conducted by: Saad Iqbal, B.A., Nicole Arabian, B.A., Robert Montgomery, M.A., Alexandra King, Ph.D., Caitlin Hibbs, B.Sc., Tonia De Barros Barreto Morton, B.A., & Lynn McFarr, Ph.D.
References
1. Harvey, S. T., & Taylor, J. E. (2010). A meta-analysis of the effects of psychotherapy with sexually abused children and adolescents. Clinical Psychology Review, 30(5), 517-535.
2. Bohus, M., Dyer, A. S., Priebe, K., Krüger, A., Kleindienst, N., Schmahl, C., Niedtfeld, I., & Steil, R. (2013). Dialectical behaviour therapy for post-traumatic stress disorder after childhood sexual abuse in patients with and without borderline personality disorder: A randomised controlled trial. Psychotherapy and Psychosomatics, 82(4), 221–233. https://doi.org/10.1159/000348451
3. Holtzhausen, L., Ross, A., & Perry, R. (2016). Working on trauma – Systematic review of TF-CBT work with child survivors of sexual abuse. Social Work/Maatskaplike Werk, 52(4). https://doi.org/10.15270/52-4-528



{kind=link}